MAPK Signaling and Angiopoietin-2 Contribute to Endothelial Permeability in Capillary Malformations
MAPK Signaling and Angiopoietin-2 Contribute to Endothelial Permeability in Capillary Malformations
Nasim, S.; Baig, M.; Wylie-Sears, J.; Vivero, M.; Smits, P.; Marrs, L.; Cheng, Y. S.; Alves, C.; Pinto, A.; Greene, A. K.; Bischoff, J.
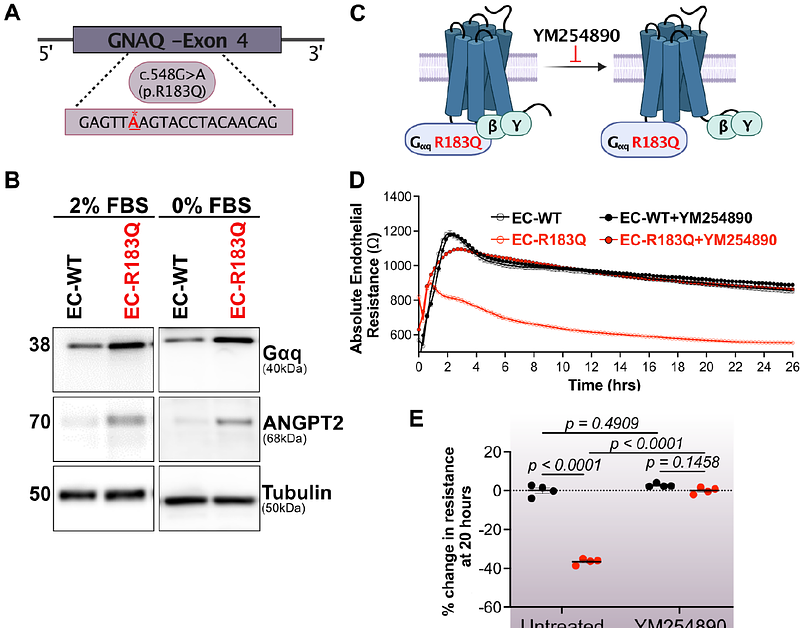
AbstractCapillary malformations (CM) are slow-flow vascular abnormalities present at birth and predominantly manifest as cutaneous lesions. In the rare neurocutaneous disorder known as Sturge Weber Syndrome (SWS), individuals exhibit CM not only on the skin but also within the leptomeninges of the brain and the choroid of the eye. >90% of CM are caused by a somatic R183Q mutation in GNAQ, the gene encoding Gq - a heterotrimeric G-protein subunit. The somatic GNAQ mutation is notably enriched in endothelial cells (ECs) isolated from CM-affected regions. Here we show blood vessels in cutaneous and leptomeningeal SWS lesions exhibit extravascular fibrin indicating a compromised endothelial barrier. Longitudinal MRI of the brain in one SWS patient further suggests vascular permeability. To explore this pathological phenotype, we employed the trans-endothelial electrical resistance (TEER) assay to measure permeability of the EC-EC barrier in vitro. Human EC CRISPR edited to create a GNAQ R183Q allele (EC-R183Q) exhibited a reduced barrier compared to mock edited EC (EC-WT). We sought to identify signaling molecules needed for EC barrier formation. Knockdown of angiopoietin-2 (ANGPT2), known to be significantly increased in EC-R183Q and in CM, partially yet significantly restored the barrier, while an anti-ANGPT2 function blocking antibody did not. We next tested the MEK1,2 inhibitor (Trametinib) because MAPK signaling is increased by GNAQ mutation. MEK1,2 inhibitors partially restored the EC barrier, implicating involvement of MAPK/ERK signaling. The combination of ANGPT2 knockdown and Trametinib significantly restored the EC barrier to near EC-WT levels. The additive impacts of ANGPT knockdown and MEK1,2 inhibition indicate the two operate in separate pathways. In summary, we discovered that GNAQ p.R183Q ECs exhibit compromised endothelial barrier formation, reflecting the compromised EC barrier in CM lesions, and that ANGPT2 knockdown combined with Trametinib effectively restores the EC-EC barrier.